

Why Dentistry Is Treating the Wrong Problem
The difference between straight teeth and a healthy system

In conventional dentistry, we have become remarkably skilled at straightening teeth and creating beautiful smiles. Yet a deeper question remains: are we truly improving our patients’ health, or are we simply correcting the final visible stage of a much larger developmental process? Building on last week’s Johnson Paper about Dr. Weston Price’s observations, this essay examines why malocclusion is rarely the disease itself—it is a symptom. Once we understand the difference between alignment and systemic health, our entire approach to care shifts.
When most people think about dentistry, they think about teeth. In my clinical experience, however, the mouth is one of the most biologically active environments in the human body, and tooth alignment is only a small part of a much larger story. Over the years, I have observed that many of the orthodontic cases I see are not problems of “bad genes” or random misfortune. They are the predictable outcomes of earlier disruptions in growth and function.
This insight first crystallized for me while rereading Dr. Weston Price’s Nutrition and Physical Degeneration—the very work I discussed in last week’s paper. Price documented, across cultures and continents, that children raised on traditional, nutrient-dense diets developed broad, well-formed jaws with ample room for all their teeth and open airways. When those same populations adopted modern, refined diets, the next generation showed narrowed palates, crowded teeth, and altered facial structure. The teeth themselves had not changed; the environment that shaped their housing had.
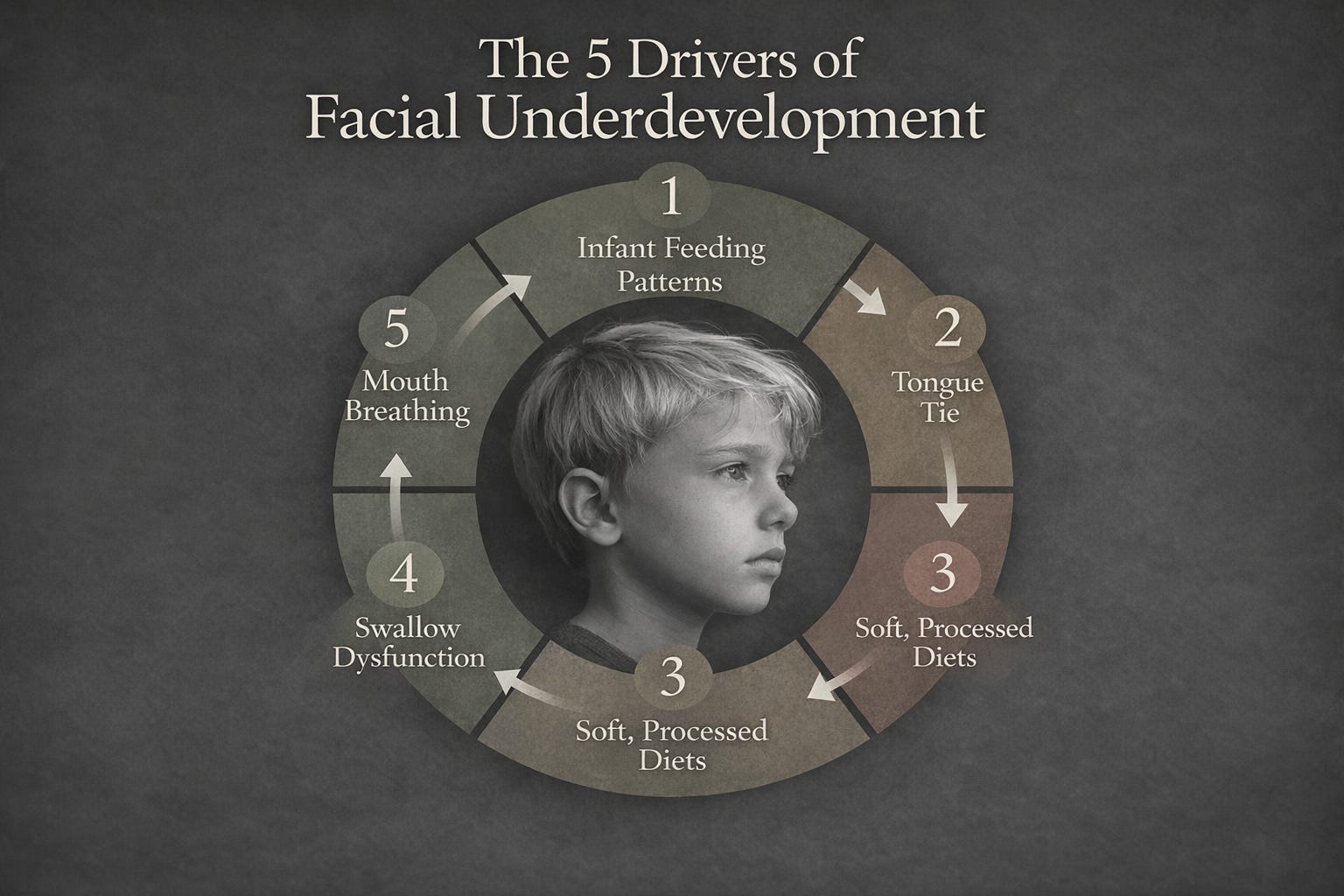
Malocclusion is the symptom, not the core disease.
In my practice, I often see this pattern. A child is not simply “a set of teeth waiting to be arranged.” A child is a developing system. Structure follows function. If the tongue does not rest properly against the palate during swallowing and at rest, the upper jaw does not receive the consistent, gentle pressure it needs for forward and lateral growth. If breathing shifts from nasal to oral—even intermittently—the tongue drops, the mandible rotates downward and backward, and the maxilla narrows. If chewing forces are reduced because of softer modern foods, the entire craniofacial complex receives less mechanical signaling for robust development.
By the time the permanent teeth erupt and crowding becomes obvious, the architectural decisions have already been made. The narrow maxilla, the recessed midface, the compromised tongue space—these are not cosmetic footnotes. They directly influence airway volume, sleep quality, and long-term systemic inflammation.
Traditional orthodontics has become extraordinarily precise at managing the visible result. We diagnose malocclusion, create space (often through extraction), retract the anterior teeth into that space, and produce a straight, pleasing smile. The before-and-after photographs are compelling. Yet in my experience, we must pause and ask a more fundamental question: what have we done to the volume of the oral cavity and the dimensions of the airway?
When we reduce the space where the tongue should live, we may improve alignment while simultaneously limiting function. Emerging research continues to explore these relationships, and while the full clinical implications are still being clarified, the pattern I have witnessed over decades is unmistakable: some patients who underwent extractions and significant retraction later report poorer sleep quality, increased nasal resistance, or myofunctional strain. These are not universal outcomes, but they appear frequently enough in biological-dentistry practices to warrant serious consideration.
This is not a criticism of orthodontics as a discipline. Orthodontists perform remarkable work and relieve real suffering. The point is more subtle: alignment alone is not the same as health. A different priority changes everything.
Instead of asking only how to fit the teeth into the existing skeletal framework, biological dentistry asks how we can support the forward growth of the face itself. We look earlier—at habits once dismissed as minor: tongue posture, nasal breathing, chewing function, and sleep quality. We recognize that these are the actual drivers of craniofacial development. When we intervene with myofunctional therapy, gentle palatal expansion, or habit-training appliances during the mixed dentition years, we are no longer simply moving teeth; we are guiding the growth trajectory of the entire system.
Many patients are surprised to discover how early these patterns begin. A history of thumb-sucking, prolonged pacifier use, or even subtle mouth breathing during allergies can set the stage for the crowded arches we later treat with braces. Once parents and practitioners see the mouth as a functional matrix rather than a set of ivory tiles, the conversation shifts from “When do we start braces?” to “How do we protect healthy growth now?”
In clinical interpretation, this perspective does not discard conventional tools—it reframes them. Straight teeth remain desirable, but they become the fortunate byproduct of a well-developed airway and balanced oral posture rather than the sole objective. The goal is no longer merely aesthetic harmony; it is a craniofacial complex that supports effortless nasal breathing, stable sleep, and lifelong systemic resilience.
For patients and families, this means asking different questions at the first orthodontic consultation: Is there adequate forward growth? Is the airway being respected? Are we addressing the functional habits that produced the crowding? For referring physicians and pediatricians, it means recognizing that a narrow palate or retrusive chin is not merely a dental curiosity—it may be an early marker of sleep-disordered breathing with downstream effects on attention, growth hormone release, and immune regulation.
We stand at an inflection point in modern dentistry. We can continue refining ever more sophisticated techniques for managing symptom generation after generation. Or we can step back and address the developmental system that produces those symptoms in the first place.
The choice is between treating teeth in isolation and supporting the whole system. Once you recognize the difference between straight teeth and true craniofacial health, it is difficult to return to previous practices.
References
Price WA. Nutrition and Physical Degeneration. 8th ed. La Mesa, CA: Price-Pottenger Nutrition Foundation; 2008. (Original work published 1939)
Kahn S, Ehrlich P. Jaws: The Story of a Hidden Epidemic. Stanford, CA: Stanford University Press; 2018.
Mew M. Tongue posture and its influence on craniofacial growth. Journal of Orthodontics. 2015;42(3):201-208.
Liu SY, et al. Myofunctional therapy for obstructive sleep apnea: a systematic review and meta-analysis. Sleep Medicine Reviews. 2023;68:101-112.
McNamara JA Jr. The role of the nasorespiratory complex in the etiology of malocclusion. American Journal of Orthodontics and Dentofacial Orthopedics. 1984;85(6):498-506.
Dr. John Johnson, DDS
Midwest BioHealth
The Johnson Papers